Surgical Risk & Complexity Analyzer
Select a procedure to analyze its risk profile, critical danger zones, and the primary challenges faced during recovery.
Heart Transplant
CABG (Bypass)
Valve Replacement
Aneurysm Clipping
Quick Facts on Surgical Risk
- Risk is measured by mortality rates (the percentage of patients who don't survive).
- Complexity depends on the organ's role; the heart and brain are the hardest to operate on.
- Patient health (comorbidities) often matters more than the surgery itself.
- Modern technology like robotic arms has lowered risks, but some procedures remain deadly.
The Heavyweight Champion of Risk: Heart Transplants
If you're looking for the peak of surgical danger, you'll find it in Heart Transplantation is a procedure where a failing heart is replaced with a healthy donor organ. Also known as Orthotopic Heart Transplantation, this isn't just a plumbing job; it's a biological war. The surgeon has to stop the heart, disconnect the life-sustaining vessels, and sew in a new organ while the patient is kept alive by a machine.
The danger here isn't just the surgery itself, but what happens after. The body's immune system is designed to attack foreign objects. Since the new heart is a "foreign object," the patient must take heavy immunosuppressants for the rest of their life. This creates a paradox: the drugs that keep the heart beating also make the patient incredibly vulnerable to infections that a healthy person would shrug off. One bad bout of pneumonia can be fatal for a transplant recipient.
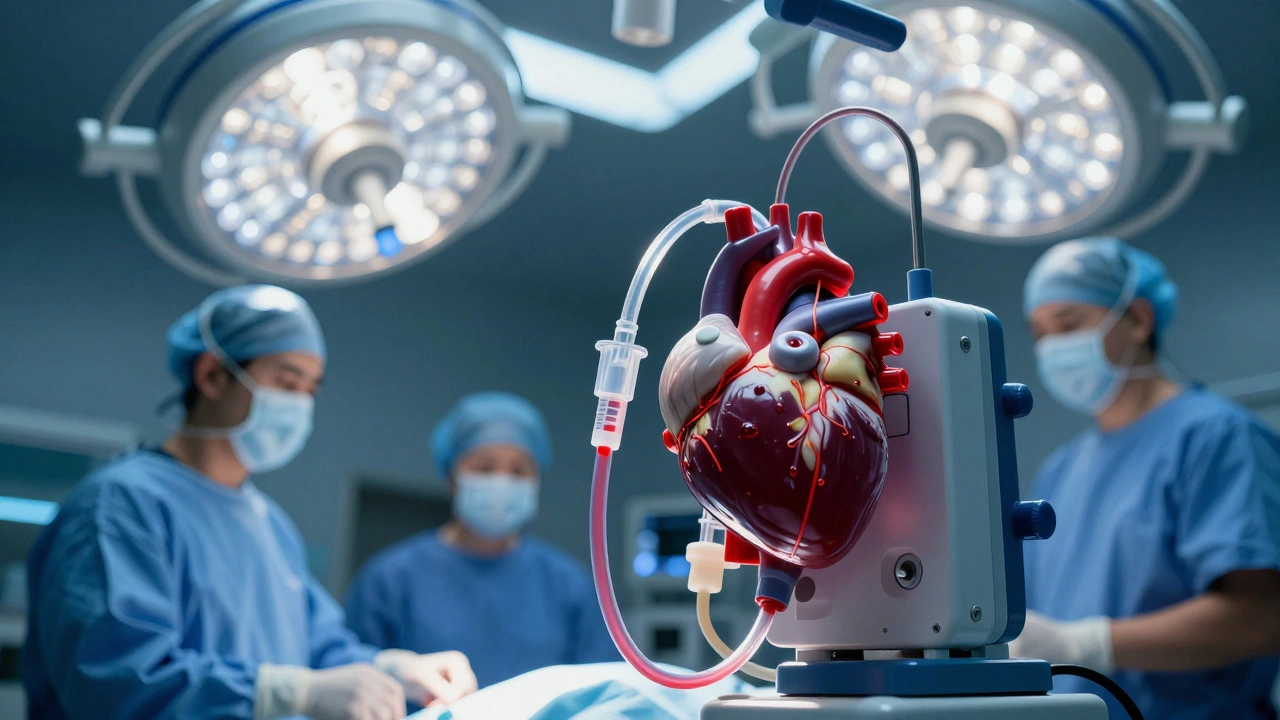
The Complexity of Open Heart Surgery
While a transplant is the extreme, Open Heart Surgery is any procedure where a surgeon opens the chest cavity to treat the heart's valves or arteries. This category includes CABG (Coronary Artery Bypass Grafting), which is one of the most common yet high-stakes operations in the world.
The real risk comes from the Heart-Lung Machine, which temporarily takes over the functions of the heart and lungs during surgery. While this machine is a lifesaver, it can cause blood clots or trigger a systemic inflammatory response. If a tiny air bubble enters the bloodstream during the process, it can travel straight to the brain, causing an immediate stroke. This is why you'll see surgeons obsessing over the "purging" of the lines before restarting the heart.
| Procedure | Primary Risk Factor | Critical Recovery Phase | Typical Complexity |
|---|---|---|---|
| Heart Transplant | Organ Rejection / Sepsis | First 90 Days | Extreme |
| CABG (Bypass) | Stroke / Heart Attack | First 2 Weeks | High |
| Valve Replacement | Blood Clots / Leakage | First Month | Moderate-High |
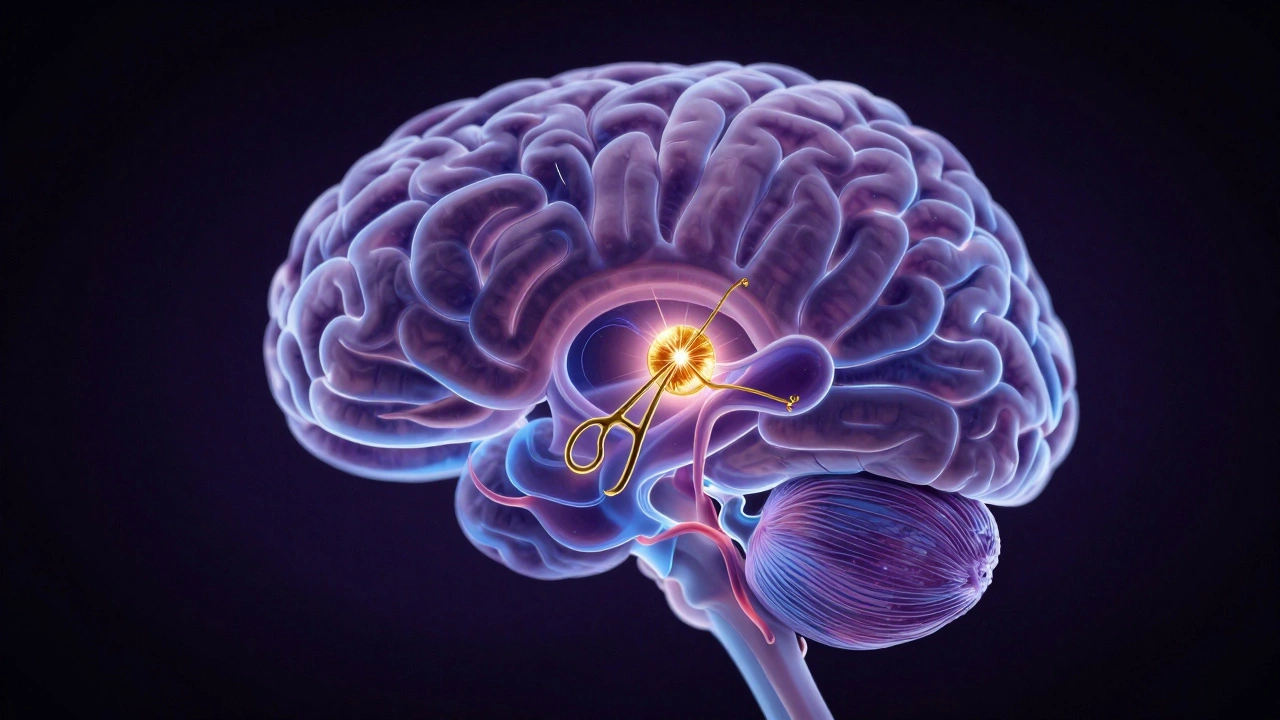
The Brain: The Other Danger Zone
We can't talk about risk without mentioning the Neurosurgery field, specifically surgeries involving the brainstem or deep cerebral tissues. Unlike the heart, which is a muscle that can be restarted, the brain consists of billions of neurons that don't regenerate. One millimeter of a slip with a scalpel can mean the difference between a patient who can speak and a patient who is permanently paralyzed.
Aneurysm clipping is particularly terrifying. A Cerebral Aneurysm is a weakened area in an artery wall that balloons out and can burst. When a surgeon goes in to clip it, they are working on a "ticking time bomb." If the aneurysm ruptures during the procedure, the resulting hemorrhage can kill the patient in seconds. It's a high-pressure environment where the surgeon is fighting against the clock and a very fragile vessel.
Why Some Surgeries Feel Riskier Than Others
It's a mistake to think that only "big" surgeries are dangerous. Risk is often a combination of the procedure and the Comorbidity of the patient. If a healthy 30-year-old has a complex surgery, their odds are great. But if an 80-year-old with chronic kidney disease and diabetes needs a heart valve replacement, the risk skyrockets.
Diabetes, for example, ruins the body's ability to heal wounds. A surgical incision that would close in a week for most people might stay open or become infected in a diabetic patient. This leads to sepsis, which is a systemic infection that causes organ failure. In many cases, the surgery is a success, but the patient dies from the "aftershocks" because their body simply couldn't handle the trauma of the operation.
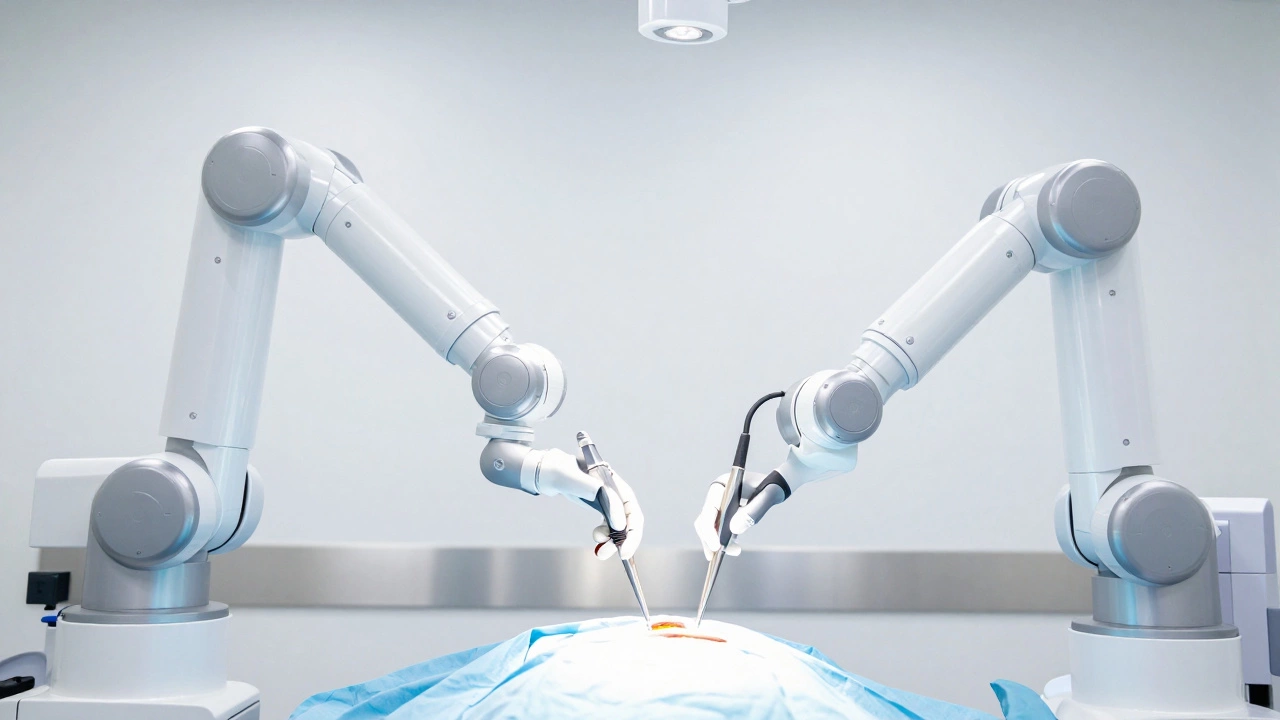
How We Make These Operations Safer
Fortunately, we aren't just guessing. The rise of Robotic Surgery, using systems like the Da Vinci System, allows surgeons to operate through tiny holes rather than wide-open incisions. This reduces blood loss and infection rates significantly. Instead of a 10-inch scar, you might have three tiny dots.
We also have better Anesthesiology. Modern anesthesia isn't just about putting you to sleep; it's about precise hemodynamic monitoring. Doctors can now track the exact oxygen saturation in your tissues and adjust blood pressure in real-time, which prevents the brain from starving for oxygen while the heart is stopped. This level of control has turned once-deadly operations into routine procedures.
The Psychological Toll of High-Risk Surgery
The risk isn't just physical. For the patient, the anxiety of a "high-risk" label can actually affect recovery. Stress releases cortisol, which can slow down the immune system. This is why many top-tier hospitals now integrate mental health support before and after major heart or brain surgeries. Helping a patient believe they will survive actually improves their physiological odds of doing so.
For the surgeons, the pressure is immense. There is a phenomenon known as "surgical fatigue" where the mental weight of losing a patient can lead to burnout. This is why the most dangerous surgeries are always performed by a team. You have the lead surgeon, the assistant, the scrub nurse, and the anesthesiologist all cross-checking each other's work. The goal is to create a system where a human error is caught before it ever reaches the patient.
Is a heart transplant more dangerous than a brain surgery?
It depends on the goal. Brain surgeries often have higher risks of permanent disability (like losing a motor function), whereas heart transplants have a higher risk of total organ failure or death due to rejection. In terms of sheer mortality over a five-year period, the transplant journey is generally more volatile due to the lifelong need for immunosuppressants.
What is the mortality rate for open heart surgery?
For routine CABG (bypass) surgery, the mortality rate is quite low, often between 1% and 3% in high-volume centers. However, if the patient is in "crash" condition or has multiple organ failures, that number can jump significantly. It's less about the surgery and more about the patient's overall health.
Can robotic surgery completely remove the risk of heart operations?
No. Robotic surgery reduces the risk of infection and blood loss because the incisions are smaller. However, the internal risks-like a blood clot forming or a valve leaking-remain. The robot is just a more precise tool; the complexity of the human heart is still the primary challenge.
Why is the heart-lung machine considered risky?
The machine replaces your natural blood flow with a mechanical pump. This can cause the blood to clot or trigger an inflammatory response from the body, which thinks the machine is a foreign invader. It can also lead to "pump head," a term for mild cognitive impairment some patients feel after their brain is perfused by a machine instead of a heart.
What happens if a surgeon makes a mistake during brain surgery?
Because the brain is mapped to specific functions, a mistake in one area can lead to a specific loss. A slip in the Broca's area might cause a loss of speech, while a mistake in the motor cortex could cause paralysis on one side of the body. This is why "awake craniotomies" are used, where the patient is woken up to talk or move while the surgeon is operating.
Next Steps for High-Risk Patients
If you or a loved one are facing a high-risk procedure, the first step is to seek a "Center of Excellence." This is a hospital that performs a huge volume of that specific surgery. Statistics show that surgeons who perform 200 of the same operation a year have much better outcomes than those who do 20. Don't be afraid to ask about the surgeon's personal success rate for your specific condition.
Pre-habilitation is also key. This means getting your body in the best possible shape before the surgery. Improving your nutrition, managing your blood pressure, and even doing light walking can increase your lung capacity and help you survive the anesthesia and recover faster. The goal is to enter the operating room with as much physiological reserve as possible.